
Cancer Is Not a Sudden Arrival—It Is a Prolonged Ambush Waiting for a Breach in the Immune Defense
June 3, 2026
Why does the same stress cause some people to thrive and become more resilient, while others become increasingly susceptible to illness?
June 3, 2026The cancers you have never developed were quietly eliminated by your immune system.
The cancers you have never developed were quietly eliminated by your immune system.
—— The Immunosurveillance Theory: A century-long legend of proposal, denial, and validation.
⏱ A One-Minute Read
Your body produces cancerous cells every day. Every cell division has a chance of error, and daily exposure to ultraviolet rays, free radicals, and metabolic byproducts continuously damages DNA. With approximately 30 billion cell divisions occurring in the human body every day, why doesn't the majority of the population develop cancer every year?
The answer is "Immunosurveillance." When this concept was first proposed in 1957, it was highly controversial; it was rejected by mainstream immunology in the 1970s, but was re-validated in the 2000s by precise experimental evidence and upgraded into today’s "Cancer Immunoediting" theoretical framework.
This is one of the most tumultuous theories in the history of immunology—its rise and fall is not just a piece of scientific history, but the core framework for understanding what your immune system does every day and why cancer eventually breaks through its defenses.
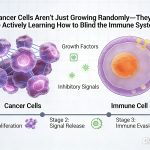
Layer 3 | Core Theory: The "Three Lines of Defense" Model of Immunosurveillance
| Defense Line | Key Effector Cells | Recognition Mechanism | Clearance Efficiency |
|---|---|---|---|
| 1st: Innate Immune Rapid Response | NK cells, $gammadelta$T cells, M1 Macrophages | NKG2D recognizes stress ligands; "Missing-self" check on MHC I | Rapid (minutes), but lower precision |
| 2nd: Innate-Adaptive Bridge | Dendritic cells (DC), NKT cells | DC captures tumor debris to activate CTL; NKT recognizes glycolipid antigens | Medium (days), initiates adaptive response |
| 3rd: Adaptive Immune Precision | CD8+ CTL, CD4+ Th1 cells | TCR recognizes tumor neoantigens presented by MHC I | Slow (1–2 weeks), highly specific, forms immune memory |
| The synergy of the three lines: The first line eliminates "obviously abnormal" early-stage cancerous cells and activates the second line by releasing inflammatory signals. The second line (DC) presents tumor debris to T cells to initiate a precise adaptive immune response. The third line (CTL) uses high specificity to target and destroy cancer cells with specific neoantigens and forms immune memory for long-term surveillance of residual cancer cells. These three lines are indispensable; the failure of any one line can allow cancer cells to enter the "equilibrium" or "escape" phases. |
Diagram: Key Research Evidence on Stress-Immunity
| 1957 - Proposal: Burnet and Thomas independently propose the "Immunosurveillance" hypothesis—under normal circumstances, the immune system eliminates large numbers of cancerous cells daily. |
| 1970s - Denial: The theory was rejected because nude mice (lacking T cells) did not show an increase in tumors. However, this was a misinterpretation caused by compensatory activity from NK cells. |
| 2001 - Rebirth: The Schreiber team used RAG2-/- mice (completely immune-deficient) to definitively confirm the existence of immunosurveillance. |
| 7Epidemiological Evidence: Organ transplant patients (after immunosuppression) have a 2-4 times higher overall cancer risk; HIV/AIDS patients have a 3,640-fold higher risk of Kaposi sarcoma. |
| Clinical Application: Enhance surveillance (prevention): regular exercise/adequate sleep/Vitamin D/vaccines against oncogenic viruses; Block escape (treatment): immune checkpoint inhibitors. |
Tier 4 | In-Depth Reading
I. Birth of the Theory: Burnet’s "Non-self" Hypothesis
In 1957, Frank Macfarlane Burnet, who later won the 1960 Nobel Prize for his Clonal Selection Theory, proposed the "Immunological Surveillance" hypothesis. He noted a paradox: if genetic mutations accumulate continuously, humans should be overwhelmed by cancer at a very young age. Yet, most people only develop cancer in old age, and most only get it once. His explanation: the immune system must be continuously monitoring and clearing early-stage cancerous cells.
However, the theory faced severe challenges in the 1970s. The development of the nude mouse model (lacking T cells) showed no significant increase in spontaneous tumors compared to normal mice. Later research revealed the fatal flaw: although nude mice lacked T cells, their NK cell function was highly potent, compensating for the T cell deficiency.
2. Rebirth: The Precise Experiments of 2001
In 2001, a heavyweight study published in the journal Nature breathed new life into the immunosurveillance theory. The Schreiber team at Washington University used a more thorough immune-deficient model than nude mice: RAG2 knockout mice. RAG2-/- mice possess neither T cells nor B cells, and their innate immune function is also significantly weakened due to the lack of lymphocytes. The experimental results were very clear: after treatment with potent chemical carcinogens, the frequency of tumor occurrence in RAG2-/- mice was significantly higher than in immune-competent wild-type mice—and the tumors appeared earlier and grew larger. Even without the application of any external carcinogens, the rate of spontaneous tumors in aging RAG2-/- mice was higher than in age-matched normal mice.
Even more convincing were the subsequent "transplantation experiments": researchers transplanted tumors grown in RAG2-/- mice into immune-competent mice, and these tumors were often rejected; however, when tumors grown in immune-competent mice were transplanted into RAG2-/- mice, they grew easily. This indicates that tumors grown in an immune-deficient environment, because they had not undergone the screening of immune pressure, retained a large number of "features identifiable by the immune system" and were rapidly cleared once placed back into an environment with an immune system. In contrast, tumors grown in a normal immune environment had already evolved the ability to escape under immune pressure. This serves as direct experimental evidence for the concept of "immunoediting."
3. Epidemiological Evidence: "Surveillance Failure" Data in the Real World
Beyond laboratory data, real-world epidemiological data provides evidence that cannot be ignored. Organ transplant patients: Large-scale epidemiological studies (the CTTR study, covering over 200,000 organ transplant patients across more than 17 countries) show that the overall cancer incidence risk after organ transplantation is 2 to 4 times higher than that of the age/sex-matched general population; the risk of non-melanoma skin cancer is increased by 65-fold, Kaposi sarcoma by 200-fold, and non-Hodgkin lymphoma by 8-fold.
HIV/AIDS patients: In AIDS patients who have not received antiviral treatment and have severely compromised immune systems (CD4+ T cells < 200/μL), the risk of Kaposi sarcoma is increased by 3,640-fold, non-Hodgkin lymphoma by 77-fold, and anal cancer by approximately 45-fold. Patients with congenital immunodeficiency syndromes (such as SCID, ataxia-telangiectasia, etc.) all show significantly higher cancer incidence rates than the general population, especially for lymphoma and leukemia. Conversely, prospective studies have found that individuals with higher peripheral blood NK cell activity have lower cancer incidence rates—all of which confirm the continuous inhibitory effect of immunosurveillance on cancer at the population level.
4. Blind Spots of Immunosurveillance: Scenarios Most Prone to Failure
Low immunogenicity tumors (low TMB): Cancers such as pancreatic cancer, prostate cancer, and low-grade gliomas have extremely low tumor mutational burden and produce very few neoantigens, leaving the immune system without enough targets to "see." Immune-privileged sites: Areas such as the brain, the anterior chamber of the eye, and the testes are inherently "dead zones for immunosurveillance"—structures like the blood-brain barrier make it difficult for systemic immune cells to enter. Cancers occurring in these regions (such as glioblastoma) can often grow quietly in an environment relatively free from immune interference.
Chronic inflammatory environments: This presents a paradox—inflammation typically activates the immune system, but long-term chronic inflammation (such as hepatitis B-related hepatitis, Helicobacter pylori-related gastritis, and inflammatory bowel disease) actually "exhausts" the efficiency of immunosurveillance while providing a microenvironment that promotes carcinogenesis. Immunosenescence: As we age, the number of NK cells declines and their function weakens, the diversity of CD8+ T cells decreases (the TCR repertoire of elderly individuals shrinks), and the proportion of Treg cells rises relatively. These characteristics of "immunosenescence" directly weaken the efficiency of tumor immunosurveillance and are one of the core immunological mechanisms underlying the increase in cancer incidence with age. After the age of 40, maintaining the overall health of the immune system is a vital foundation for sustaining tumor surveillance efficiency.
5. Clinical Implications of the Immunosurveillance Theory
Understanding the immunosurveillance theory points directly to two different approaches for cancer prevention and treatment. Enhancing surveillance efficiency (primarily for cancer prevention): Maintaining the healthy function of NK cells and CTLs is the core of primary prevention. Evidence-supported strategies include: regular moderate-to-high intensity aerobic exercise (which increases NK cell numbers and cytotoxic activity); adequate sleep (sleep deprivation directly impairs NK cell function; a 2019 study in Nature Communications showed that losing 4 hours of sleep in one night led to a ~70% drop in NK cell activity the following day); sufficient Vitamin D; and vaccination against known oncogenic viruses (HPV, Hepatitis B).
Blocking escape (primarily for cancer treatment): When cancer has already broken through immunosurveillance and entered the "escape" phase, the goal of treatment is no longer to "enhance" an already suppressed immune system, but to "block the tumor's escape mechanisms"—this is the exact logic behind immune checkpoint inhibitors. PD-1/PD-L1 inhibitors do not "boost" the immune system; instead, they "release the brakes" installed by the tumor, allowing already present but suppressed CTLs to function again. Between these two lies "intervention in the equilibrium phase"—if the equilibrium phase can be identified via ctDNA liquid biopsy, it may be possible to conduct "preventive immune intervention" before the cancer formally escapes, which is the core focus of future research on early cancer immune intervention.
6. Practical Implications for Personal Health Management
The most important practical implication of the immunosurveillance theory for the average person is that it shifts the mental framework of "cancer prevention." Traditional cancer prevention focuses on reducing "carcinogenic exposure"—quitting smoking, using sunscreen, and avoiding carcinogens. These remain important. However, the immunosurveillance theory adds another dimension: it is equally important to maintain the immune system's ability to clear cancerous cells. This "subtraction and addition" approach forms a more complete strategy for cancer prevention.
Age is the most uncontrollable factor weakening immunosurveillance. However, the rate of immunosenescence is significantly influenced by lifestyle. At the same age of 70, individuals who engage in regular exercise, get adequate sleep, and maintain a healthy weight can have substantially better NK cell function and T cell diversity compared to those who are sedentary, chronically sleep-deprived, or obese. This means that the maintenance of immunosurveillance is not just a concern for one's youth, but a long-term investment that needs to be continued into old age. In this sense, a "healthy lifestyle" is not just about reducing carcinogenic exposure, but also about actively maintaining your body's anti-cancer defense line.
The ultimate logic of maintaining immunosurveillance is to transform "not getting cancer" from a passive "game of luck" into something where you can actively influence the probabilities. No one can guarantee 100% that they will not develop cancer, but every choice made to improve the efficiency of immunosurveillance shifts the odds in a better direction.
After the age of 40, the significance of active screening can also be understood from the perspective of the immunosurveillance theory: as immunosenescence enters an accelerated phase, those "silent" tumors long suppressed during the equilibrium phase have a greater chance of entering the escape phase. This is why many screening programs are initiated between the ages of 40 and 50—not just because of accumulated mutations, but also because immunosurveillance is beginning to lag. Regular screening is a way to supplement this defense line with artificial means during the stage of life when immunosurveillance efficiency declines.
Key Takeaways
- Theory Evolution: The immunosurveillance theory, proposed by Burnet and Thomas in 1957, underwent a period of "denial" in the 1970s (due to misinterpretations of nude mouse experiments) before being "reborn" following the 2001 $RAG2^{-/-}$ mouse experiments by the Schreiber team. This history serves as a classic case study of how science progresses through self-correction.
- Evidence: The three lines of defense in immunosurveillance work synergistically to clear massive numbers of cancerous cells daily. Epidemiological data from organ transplant recipients (2–4 fold increase in cancer risk) and HIV/AIDS patients (tens to thousands of fold increase in specific cancers) provide the strongest evidence for the existence of this surveillance.
- Blind Spots: There are four major blind spots in immunosurveillance: low immunogenicity tumors (low TMB), immune-privileged sites (brain, eyes, testes), chronic inflammatory environments, and immunosenescence (declining NK cell function). Maintaining immune health after age 40 is key to delaying the decline in surveillance efficiency.
- Applications: "Enhancing surveillance" (cancer prevention) and "blocking escape" (cancer treatment) represent two different levels of application: the former relies on regular exercise, adequate sleep, Vitamin D, and oncogenic virus vaccines, while the latter relies on "releasing the brakes" via immune checkpoint inhibitors.
- Frontiers: "Equilibrium phase intervention"—identifying and intervening before a cancer formally escapes—is the current frontier in tumor immunology. This approach depends on highly sensitive technologies like ctDNA liquid biopsy and holds the promise of ushering in a new era where cancer is eliminated before it can fully form.
FAQ | Questions You're Most Likely to Ask
Core Sources Cited
-
Burnet FM (1957). Cancer: a biological approach. British Medical Journal, 1(5022), 841–847.
-
Shankaran V et al. (2001). IFNγ and lymphocytes prevent primary tumour development. Nature, 410, 1107–1111.
-
Vajdic CM & van Leeuwen MT (2009). Cancer incidence after solid organ transplantation. International Journal of Cancer, 125(8), 1747–1754.
-
Imai K et al. (2000). Natural cytotoxic activity of peripheral-blood lymphocytes and cancer incidence. The Lancet, 356, 1795–1799.
-
Schreiber RD et al. (2011). Cancer immunoediting. Science, 331(6024), 1565–1570.

{kind=link}
{kind=link}
{kind=link}