
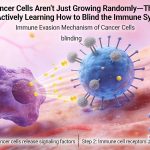
Cancer Cells Aren’t Just Growing Radomly—They Are Actively Learning How to Blind the Immune System
June 3, 2026
The cancers you have never developed were quietly eliminated by your immune system.
June 3, 2026Cancer Is Not a Sudden Arrival—It Is a Prolonged Ambush Waiting for a Breach in the Immune Defense
Cancer Is Not a Sudden Arrival—It Is a Prolonged Ambush Waiting for a Breach in the Immune Defense
—— The Intersection of Immune Senescence, NK Cells, and Tumor Immunoediting
⏱ A One-Minute Read
For individuals over the age of 60, the incidence of cancer is nearly 10 times higher than that of those aged 20 to 40. Why? The accumulation of genetic mutations with age is one reason. However, there is another reason that is severely underestimated in public discourse: as age increases, the immune system's capacity to surveil and clear away cancerous cells undergoes a systemic decline. Your body produces cancerous cells every day, and it clears them away every day as well. In this war, the immune system wins easily during youth; as age advances, the defensive line grows increasingly thin, and more and more cells slip through the net. The relationship between age and cancer is half about the accumulation of mutations, and half about the aging of the surveyors. Only by understanding both halves can one comprehend why maintaining immune surveillance capacity holds real, actionable significance for cancer prevention.
Level 3 | Core Theory: The Six Immune Evasion Strategies of Cancer Cells
| Mechanism | Content |
|---|---|
| Dual Superposition of Mutation Accumulation × Surveillance Decline | Decades of accumulated DNA damage increase the probability of cellular malignant transformation. Concurrently, the efficiency of immune surveillance declines (decreased NK cell activity, reduced T-cell diversity), resulting in a simultaneous drop in the clearance probability of existing cancerous cells. |
| Acceleration of the "Escape" Phase in Immunoediting | Under long-term selective pressure from the immune system, cancerous cells capable of immune evasion are selected and preserved. In older adults, weakened immune pressure lowers the threshold for the expansion of these evasive cells, making it easier to break the "equilibrium" phase and progress into the "escape" phase. |
| Inflammaging Providing a Pro-Growth Environment for Tumors | Persistent, low-grade chronic inflammation (inflammaging) supplies the tumor microenvironment with pro-angiogenic and pro-invasive signals (such as IL-6 and TNF-α) while simultaneously suppressing effective anti-tumor immune responses. |
| The elevated risk of cancer in older adults is not simply a matter of "damaged cells" acting alone, nor is it solely a matter of "weakened immunity." Instead, it is the result of these two events occurring simultaneously and compounding each other. Only by understanding this superposition can one comprehend the real significance of maintaining immune surveillance capacity. |
Tier 4 | In-Depth Reading
I. The Cancer-Age Curve: The Most Direct Epidemiological Evidence
If you plot the age-specific incidence of various cancers worldwide (lung, colorectal, breast, prostate, gastric, etc.), almost all the curves exhibit the same shape: before the age of 40, incidence remains relatively low; after 40, the curve begins to curl upward; after 60, it rises sharply; and above 80, it reaches its peak.
Data from the National Cancer Institute (NCI) indicates that cancers diagnosed in the 60–79 age group account for approximately 45% of all cancer cases, even though this age group makes up only about 20% of the total population.
For a long time, this age distribution was primarily attributed to the accumulation of mutations—every time a cell divides, there is a certain probability of DNA replication errors. Decades of this accumulation make it easier for the multiple mutations required for oncogenesis to appear simultaneously. This explanation is correct, but incomplete.
If there were only an accumulation of mutations without a concurrent decline in immune surveillance, many of these mutation-laden cells would still be cleared by the immune system—just as they were during youth. The sharp uptick in the cancer-age curve coincides perfectly with the time point when immunosenescence becomes prominent, and this is no coincidence.
2. NK Cells: The Front Line of Cancer Surveillance and the Most Apparent Site of Aging
In the immune system's battle against cancer, Natural Killer (NK) cells are the most critical component of innate immunity. They do not need to pre-learn specific tumor antigens to recognize and kill cancerous cells—especially those that downregulate MHC-I (Major Histocompatibility Complex Class I) molecules to evade T cells. Instead, NK cells identify them through the "missing-self" mechanism.
While the number of NK cells in older adults may increase compensatorily, their quality declines systemically. This drop in quality has a direct impact on cancer surveillance:
- NKG2D receptor expression declines with age: As this critical receptor for recognizing stress signals on cancerous cells wanes, the efficiency of detecting cellular "distress signals" decreases.
- Perforin and granzyme contents diminish with age: With fewer of these "weapons" used to kill target cells, the actual destructive capacity of individual NK cells drops.
- Proliferation and persistence capacities after activation decline: This makes it difficult to maintain continuous surveillance pressure.
A long-term follow-up study published in The Lancet tracked over 11,000 middle-aged and elderly participants, measuring their natural killer cell activity (NKCA), and followed them for 11 years. The results showed that individuals in the lowest quartile of baseline NKCA had a cancer incidence approximately 1.7 times higher than those in the highest quartile. NK cell activity stands as an independent predictor of cancer risk.
From an epidemiological perspective, this finding directly supports the conclusion that maintaining NK cell activity makes a genuine contribution to cancer prevention. The decline in NK cell activity is an independent mechanism driving the elevated cancer risk in older adults, rather than a mere byproduct of mutation accumulation.
There is a clear chain of causality from epidemiology to molecular mechanisms linking NK cell activity to cancer risk. This forms the most vital scientific foundation for NK cell therapies in the fields of anti-aging and cancer prevention.
3. Disruption of the "Equilibrium" Phase in Immunoediting: The Unique Vulnerability of Older Adults
The theory of "cancer immunoediting" dictates that cancerous cells and the immune system go through three phases: Elimination → Equilibrium → Escape.
During the "equilibrium" phase, cancerous cells are not completely eliminated, but they are held in check by the pressure of the immune system and cannot expand. This amounts to a "cold war" between the immune system and the tumor, which can be maintained for years or even decades without clinical symptoms.
The problem is that sustaining this equilibrium requires the immune system to continuously exert sufficient pressure. As age advances and immune pressure weakens, this balance is broken more easily, entering the "escape" phase where cancer cells begin to expand unchecked and clinically detectable tumors form.
This mechanism explains a common clinical observation: many cancers in older adults are found during autopsies or incidental imaging examinations to have existed for quite some time without causing any symptoms during the patient's life. These cancers likely resided in an "equilibrium" state for a long duration, only progressing rapidly when the balance was disrupted at a specific point—possibly when the immune system was weakened by other factors such as surgery, infection, or severe stress.
Understanding this mechanism carries an important practical implication: maintaining immune system pressure through lifestyle and medical interventions can prolong the "equilibrium" phase, thereby delaying or even preventing the onset of the "escape" phase.
4. Inflammaging: The "Breeding Ground" for Tumors
Inflammaging is not just a marker of immunosenescence; it is also a promoter of tumor development. Chronic low-grade inflammation provides a highly advantageous microenvironment for tumors:
- IL-6: Promotes tumor cell proliferation and survival via the JAK-STAT3 pathway, drives tumor angiogenesis, and suppresses effective anti-tumor T-cell responses.
- TNF-$\alpha$: When present continuously at low levels (unlike acute high levels), it promotes tumor cell proliferation and invasion, and participates in the polarization of M2 macrophages within the tumor microenvironment.
- Persistent NF-$\kappa$B activation: Provides anti-apoptotic protection to tumor cells, making them harder to kill.
This also serves as part of the mechanistic basis for why lowering chronic inflammation levels through an anti-inflammatory lifestyle exerts a protective effect against cancer risk—it does not kill cancer cells directly, but rather reduces the hospitable growth environment provided to them.
5. Cancer Screening: The Need for Active External Surveillance When Immune Defenses Weaken
Since the immune system's capacity for cancer surveillance declines with age, the most direct compensatory strategy at the medical level is to use artificial cancer screening to partially replace the weakened natural surveillance.
Cancer screening aims to detect the presence of cancer through testing while it is still in the "equilibrium" phase and asymptomatic, allowing for intervention before it enters the "escape" phase. Early detection means lower treatment difficulty, better efficacy, and higher survival rates.
For individuals over the age of 50, the cancer screening programs with the strongest evidence include:
-
- Colorectal Cancer Screening: Colonoscopy (every 10 years, or more frequently if indicated) or fecal occult blood testing (every 1–2 years).
- Lung Cancer Screening: Low-dose CT screening is recommended for individuals aged 50–80 with a heavy smoking history (20 pack-years or more).
- Breast Cancer Screening: Mammography for women aged 40–74, every 1–2 years.
- Cervical Cancer Screening: HPV testing for women aged 25–65, every 5 years (either alone or co-testing with cytology).
- Prostate Cancer: The indications for PSA testing remain debated; it is recommended to discuss individual risks with a doctor before deciding.
6. Maintaining NK Cell Activity: A Continuum from Prevention to Treatment
From the perspective of cancer risk prevention, maintaining NK (natural killer) cell activity is a goal supported by well-defined mechanisms. On the therapeutic side, NK cell therapy represents a rapidly evolving direction in immuno-oncology.
On the Prevention End: Regular, moderate-intensity exercise is currently the most well-evidenced lifestyle intervention for maintaining NK cell activity in older adults. Studies consistently demonstrate that older adults who exercise regularly have significantly higher NK cell cytotoxicity than their sedentary peers, with differences reaching up to 20% to 30%. This gap carries substantial significance regarding cancer risk.
On the Treatment End: NK cell therapies—including allogeneic NK cell infusions and CAR-NK cells—are showing promise in clinical trials for various hematologic malignancies and certain solid tumors. For elderly cancer patients, one potential advantage of NK cell therapy is its ability to partially bypass the limitations of diminished T-cell responses in older individuals. NK cells do not rely on MHC-I to recognize target cells, offering a complementary advantage against tumors that T cells fail to recognize efficiently.
The Continuum Prevention and treatment exist along a continuous spectrum. Maintaining immune surveillance and delaying the disruption of equilibrium belongs to the prevention end; once that equilibrium is broken and a tumor emerges, utilizing NK cell therapy to enhance immune attack represents the treatment end. Understanding this continuum is the key to connecting the biological value of NK cells with their clinical utility.
Diagram: The Relationship Between Age, Immune Surveillance, and Cancer Risk
| Age Group | Mutation Accumulation |
|---|---|
| 20–39 years old | Low |
| 40–59 years old | Moderate accumulation |
| 60–74 years old | High accumulation |
| 75+ years old | Severe accumulation |
Key Takeaways
- The elevated cancer risk in older adults is a dual superposition: the accumulation of DNA mutations (increased probability of malignant transformation) + the decline of immune surveillance (decreased probability of clearance). The two occur simultaneously and amplify each other.
- NK cell activity (NKCA) is an independent predictor of cancer risk: an 11-year follow-up study demonstrated that the cancer incidence in the lowest NKCA group was approximately 1.7 times higher than that in the highest group.
- Sustaining the "equilibrium" phase of immunoediting requires continuous immune pressure; as immune pressure weakens in older adults, this balance is broken more easily, lowering the threshold for cancer cell expansion.
- Inflammaging supplies a pro-growth environment for tumors (via IL-6, TNF-$\alpha$, and NF-$\kappa$B), and reducing chronic inflammation serves as a systemic approach to suppressing this "pro-cancer breeding ground."
- Cancer screening is the most direct medical compensation once immune surveillance weakens—detecting a tumor during the equilibrium phase yields far better treatment outcomes than waiting until the escape phase.
- Exercise stands as the lifestyle intervention with the most evidence for maintaining NK cell activity in older adults, while NK cell therapy serves as a medical means to directly enhance surveillance capabilities on the treatment side.
FAQ | Questions You're Most Likely to Ask
Core Sources Cited
-
Hanahan D & Weinberg RA (2011). Hallmarks of cancer: the next generation. Cell, 144(5), 646–674.
-
Topalian SL et al. (2012). Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. NEJM, 366, 2443–2454.
-
Fridman WH et al. (2012). The immune contexture in human tumours. Nature Reviews Cancer, 12, 298–306.
-
Mariathasan S et al. (2018). TGFβ attenuates tumour response to PD-L1 blockade. Nature, 554, 544–548.
-
Dunn GP et al. (2004). Cancer immunoediting and the three Es. Annual Review of Immunology, 22, 329–360.

{kind=link}
{kind=link}
{kind=link}