
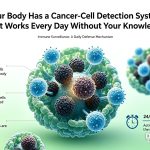
Your Body Has a Cancer-Cell Detection System That Works Every Day Without Your Knowledge
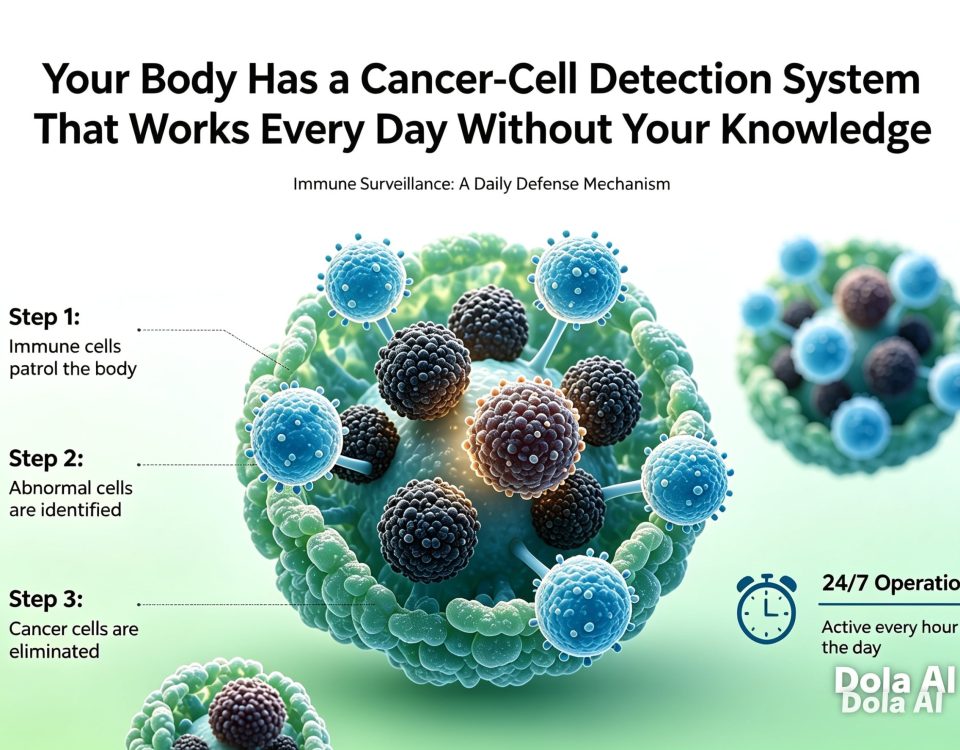
6 月 16, 2026Cancer Cells Don't Just Grow Randomly—They Actively Learn How to Make the Immune System Look the Other Way
Cancer cells aren’t just growing randomly—they are actively learning how to make the immune system turn a blind eye to them.
—— Immune Evasion: The Six Survival Strategies Evolved by Tumors
层级四|深度阅读
I. Survivorship Bias: The Tumors That Grow Are the Masters of Escape
This is the most important cognitive framework for understanding immune evasion. The immune system clears countless cancerous cells every day, but it does more than just clear them—it unknowingly performs natural selection on the tumor cell population. The cells that were easily recognized and cleared died, while those that happened to develop mutations making them harder to detect survived.
This is the essence of the "Escape" phase in "Immunoediting": a cancer cell population capable of forming a clinically visible tumor is already an elite survivor shaped by years of selective pressure from the immune system. They do not survive randomly; they happen to have evolved the most effective immune evasion strategies. This perspective fundamentally changes our understanding of tumors: a tumor's ability to evade the immune system is not an innate property, but an acquired capability evolved under immune pressure. This also means that if we attack a tumor with immunotherapy, the tumor will continue to evolve, attempting to bypass new pressures—which is one of the fundamental reasons for resistance to immunotherapy.
2. PD-L1: The Most Important "Immune Off-Switch"
Among all immune evasion mechanisms, PD-L1 (Programmed Death-Ligand 1) is the most thoroughly studied and widely applied target in clinical practice. PD-1 (Programmed Cell Death Protein 1) is a receptor on the surface of T cells. Its normal function is to "put on the brakes" for T cells after an immune response is complete, preventing the immune reaction from being overactivated and damaging healthy tissues. When a T cell's PD-1 binds to its ligand, PD-L1, the T cell enters a state of "exhaustion": it stops proliferating, stops releasing cytokines, and stops killing.
Cancer cells have discovered this mechanism and learned to exploit it. Many tumor cells (as well as macrophages co-opted by tumors) express high levels of PD-L1 on their surface. When a tumor-specific T cell finally finds the tumor and approaches it to launch an attack, it finds that the PD-L1 on the tumor cell surface binds to its own PD-1—the brakes are locked, and the T cell is turned off at the final step before reaching its target. This is why anti-PD-1 and anti-PD-L1 antibodies (such as Pembrolizumab, Nivolumab, and Atezolizumab) have produced such remarkable clinical results: they block the binding of PD-1 and PD-L1, lift the blockade on the T cells, and allow the trapped T cells to reactivate and launch an attack.
3. MHC-I Downregulation: Blinding T Cells, but Leaving a Handle for NK Cells
Many tumors evade T-cell recognition by downregulating MHC-I, a common occurrence in many tumor types, including lung cancer, colorectal cancer, and melanoma. However, MHC-I downregulation inadvertently triggers the NK cell's "missing self" recognition mechanism. Tumors face a dilemma: keep MHC-I, and T cells can see them; downregulate MHC-I, and NK cells will come after them.
Tumors have evolved an ingenious solution—upregulating a non-classical MHC-I molecule called HLA-E. HLA-E can bind to the inhibitory receptor (NKG2A) on NK cells, leading the NK cells to believe that "the ID card exists," thereby letting the tumor cells pass. This is an excellent example of the subtlety of tumor evolution: it does not simply downregulate all MHC molecules but selectively removes the parts that allow for T-cell recognition while retaining the parts that satisfy NK cells. Anti-NKG2A monoclonal antibodies (such as Monalizumab) are designed specifically to block this escape path and are currently in clinical trials.
4. How Tumors Co-opt the Immune System into an Accomplice
The most shocking immune evasion mechanism is not making the immune system "blind" to the tumor, but making the immune system actively help the tumor grow. In the tumor microenvironment, there is a class of cells called Tumor-Associated Macrophages (TAMs). Under normal circumstances, macrophages have two functional polarities: M1 (pro-inflammatory, tumor-killing) and M2 (anti-inflammatory, promoting tissue repair). Tumors release specific signals (such as IL-4, IL-13, TGF-β, and CSF-1) that drive macrophages around the tumor to polarize into the M2 phenotype. M2 macrophages do not attack the tumor; instead, they secrete factors that promote angiogenesis (VEGF), matrix metalloproteinases that promote tumor invasion, and suppress the activity of T cells and NK cells.
Similarly, Treg cells (regulatory T cells) act as the "brakes" in the normal immune system to prevent excessive activation. Tumors secrete chemokines to attract Treg cells into the tumor microenvironment, using them to suppress the activity of tumor-specific T cells. Tumors borrow weapons from the immune system around them to suppress their own resistance. This ability to co-opt is one of the reasons why mature tumors are the most difficult to overcome with immunotherapy—it is not enough to just reactivate immune attacks; one must also clear or reprogram the immune cells that have already become accomplices.
5. TGF-β: The Tumor's Universal Immune Suppression Tool
Among all the immune-suppressive factors secreted by tumors, TGF-β (Transforming Growth Factor-beta) is the most widely used and far-reaching. In the tumor microenvironment, TGF-β is a multi-target immune suppression machine: it directly inhibits NK cell activity (including downregulating the activating receptor NKG2D on the surface of NK cells); inhibits the proliferation and cytotoxic function of CD8+ T cells; drives the polarization of macrophages toward the M2 phenotype; promotes the development of Treg cells; and inhibits the maturation of dendritic cells, impacting tumor antigen presentation.
TGF-β can interfere with almost every aspect of the immune system's anti-tumor response. A 2018 study published in Nature (Mariathasan et al.) found that in bladder cancer patients, TGF-β does not just suppress the function of immune cells; it also traps T cells in the fibrous tissue surrounding the tumor, physically preventing them from entering the tumor core—this is direct evidence of the multi-layered mechanism of TGF-β in tumor immune evasion. Blocking the TGF-β pathway, in combination with other immunotherapies, holds the potential to synergistically enhance anti-tumor effects, and several combination therapies are currently in clinical trials.
6. Understanding Escape is a Prerequisite for Designing Treatment
Every immune evasion mechanism is a potential therapeutic target. Cancer cells use PD-L1 to turn off T cells → use anti-PD-1/PD-L1 antibodies to turn them back on; cancer cells use HLA-E to inhibit NK cells → study NKG2A inhibitors to remove the blockade on NK cells; cancer cells downregulate MHC-I to avoid T cells → NK cell therapies have an advantage in these types of tumors; tumors co-opt macrophages → target CSF-1R to clear M2-type macrophages, or repolarize them into the M1 phenotype.
However, reality is far more complex than this "one-to-one" logic. Mature tumors often use multiple evasion mechanisms simultaneously, and targeting just one is often only partially effective, as the tumor will quickly escape through other paths. This is why combination therapy strategies are increasingly used in clinical practice—striking multiple escape paths simultaneously to block the tumor's retreat. What is most likely to change the landscape of cancer treatment in the future is not a single "miracle drug," but the design of personalized combination therapy plans based on a precise analysis of the immune evasion mechanisms of each patient's tumor.
7. Immune Evasion and Prevention: What Can We Learn from the Mechanisms?
The theory of immune evasion does not just explain "why cancer occurs"; it also, to a certain extent, points toward "what can reduce the chances of tumor escape."
Reducing chronic inflammation is one of the core strategies. Chronic inflammation provides an ideal environment for escape by driving M2 polarization and Treg enrichment—this is why chronic hepatitis B, Helicobacter pylori infection, and chronic inflammatory bowel disease are highly associated with the risk of specific cancers; it is not just because inflammation drives mutations, but because inflammation creates an immune microenvironment favorable to escape. Eradicating H. pylori, receiving the hepatitis B vaccine, and managing inflammatory bowel disease directly reduce the formation of this inflammatory environment conducive to escape at the source.
Maintaining a healthy weight is of particular importance for preventing immune evasion. Obesity (especially excessive visceral fat) systematically increases the secretion of pro-inflammatory factors like IL-6 and TNF-α, while also increasing the production of TGF-β and adenosine, all of which are key factors that help tumors establish an immune-evasive microenvironment. Research shows that the function of NK cells in obese individuals is significantly weakened, resulting in lower efficiency in killing cancer cells. Weight loss has a direct restorative effect on NK cell function; this is not a metaphor, but a physiological change that can be measured through mechanisms.
Not smoking takes on more concrete meaning within the framework of immune evasion. Tobacco compounds are not just direct carcinogens; they also downregulate the expression of the NKG2D receptor on the surface of NK cells, directly weakening the "danger signal" recognition system; simultaneously, they upregulate the secretion of TGF-β in the tumor microenvironment, creating a more favorable environment for tumor cell escape. This means: quitting smoking is not just about reducing the chances of genetic mutations, but also about restoring the immune system's ability to recognize and attack existing mutated cells.
For patients already diagnosed with cancer, understanding the evasion mechanisms of their own tumors helps them more actively participate in discussions about treatment decisions. Asking doctors, "What is the PD-L1 expression level of my tumor?" "Is there T-cell infiltration in the tumor tissue?" "Is the TMB (Tumor Mutational Burden) high or low?"—the answers to these questions directly influence which immunotherapy regimen is most likely to be effective for you.
Key Takeaways
-
Cancer cells capable of developing into tumors are survivors screened by immune selective pressure, having evolved multiple immune evasion mechanisms—this is survivorship bias, not luck.
-
PD-L1 is the most critical "immune off-switch": tumor cells use it to directly deactivate approaching T cells, which is precisely why anti-PD-1/PD-L1 therapies have achieved such tremendous clinical success.
-
Downregulation of MHC-I blinds T cells but triggers NK cells—tumors have evolved to selectively retain HLA-E to counter both, a dual immune evasion strategy; the corresponding target is the anti-NKG2A monoclonal antibody.
-
Tumors can co-opt immune cells (such as macrophages and Tregs) into becoming accomplices, which is more dangerous and harder to combat than simply making the immune system "blind."
-
TGF-β is a "universal immunosuppressant" secreted by tumors that simultaneously suppresses NK cells, T cells, and dendritic cells, making it an important therapeutic target under research.
-
Every evasion mechanism equals a therapeutic target. The future of immunotherapy lies in combination strategies that simultaneously block multiple escape pathways.
FAQ | 你最可能问到的问题
引用来源
-
Hanahan D & Weinberg RA (2011). Hallmarks of cancer: the next generation. Cell, 144(5), 646–674.
-
Topalian SL et al. (2012). Safety, activity, and immune correlates of anti-PD-1 antibody in cancer. NEJM, 366, 2443–2454.
-
Fridman WH et al. (2012). The immune contexture in human tumours. Nature Reviews Cancer, 12, 298–306.
-
Mariathasan S et al. (2018). TGFβ attenuates tumour response to PD-L1 blockade. Nature, 554, 544–548.
-
Dunn GP et al. (2004). Cancer immunoediting and the three Es. Annual Review of Immunology, 22, 329–360.

{kind=link}
{kind=link}
{kind=link}